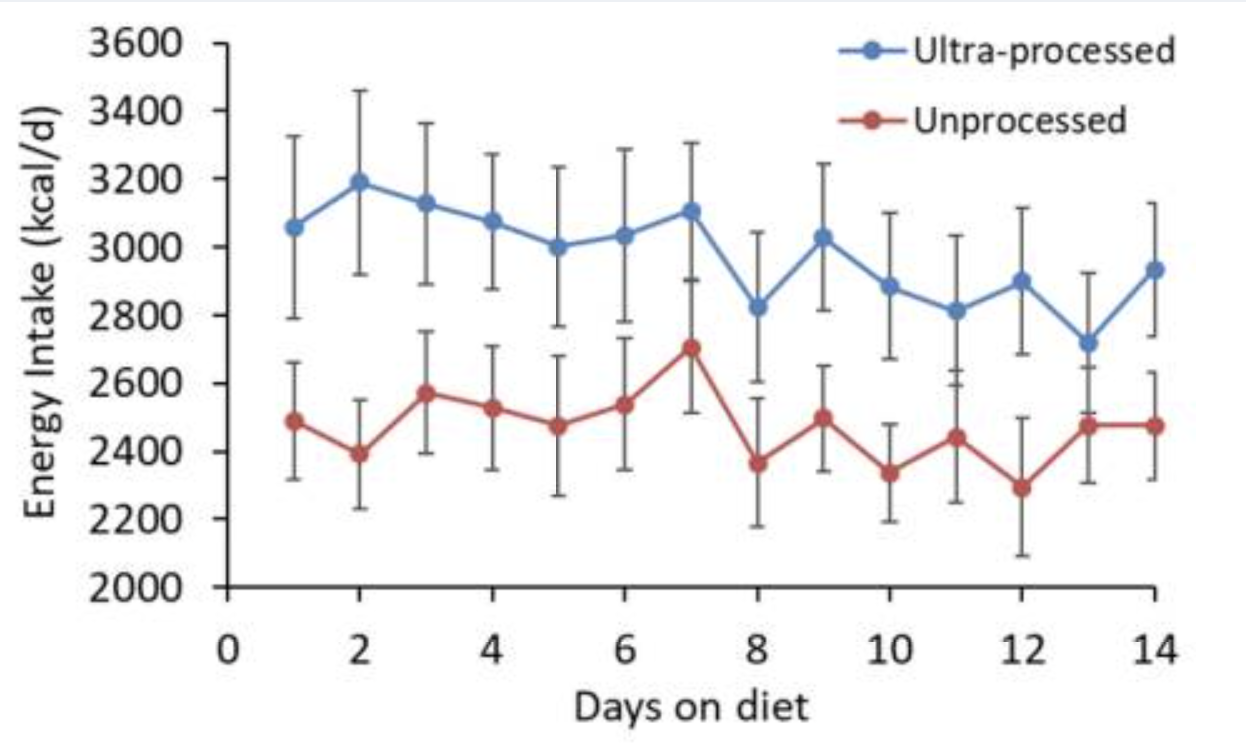
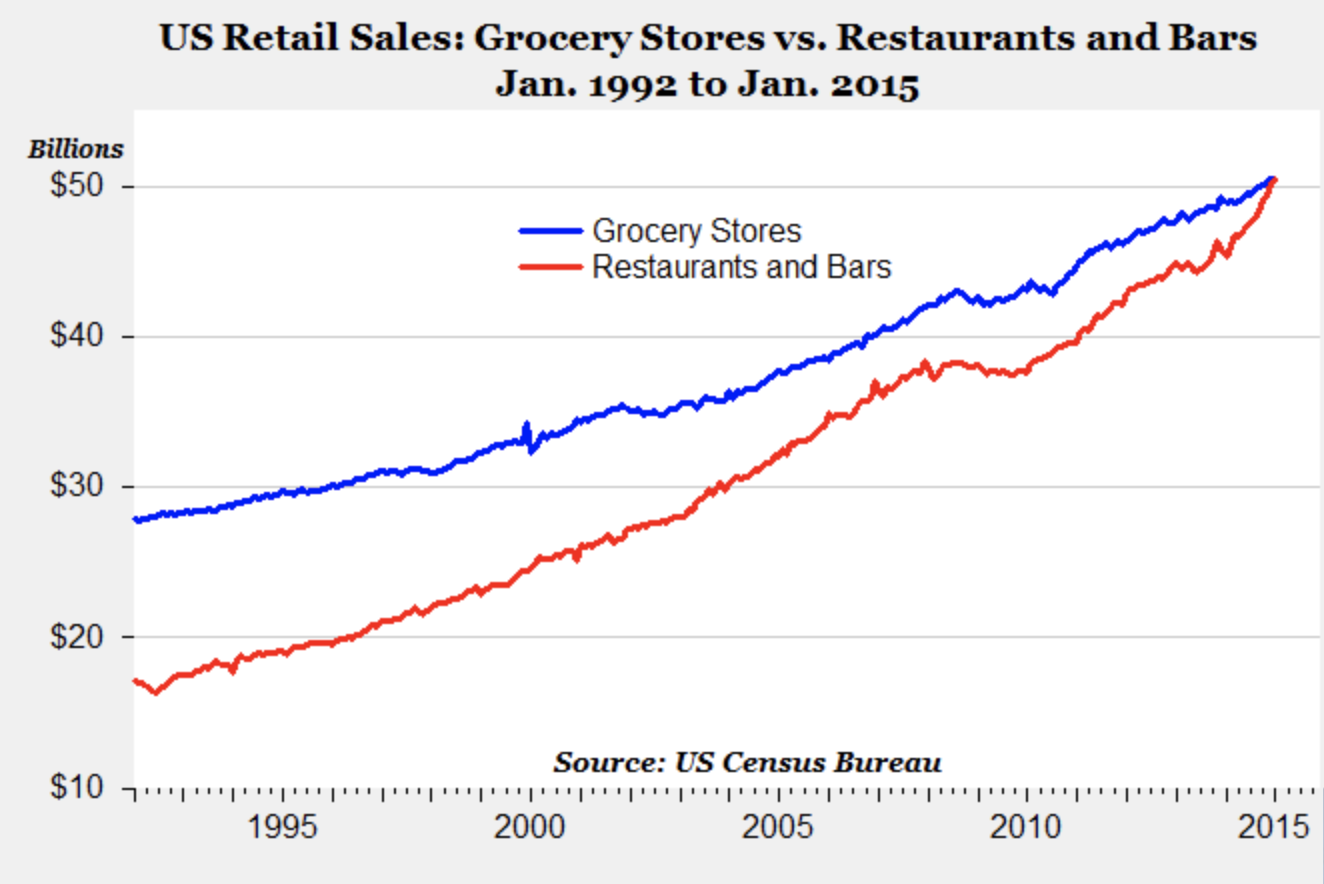
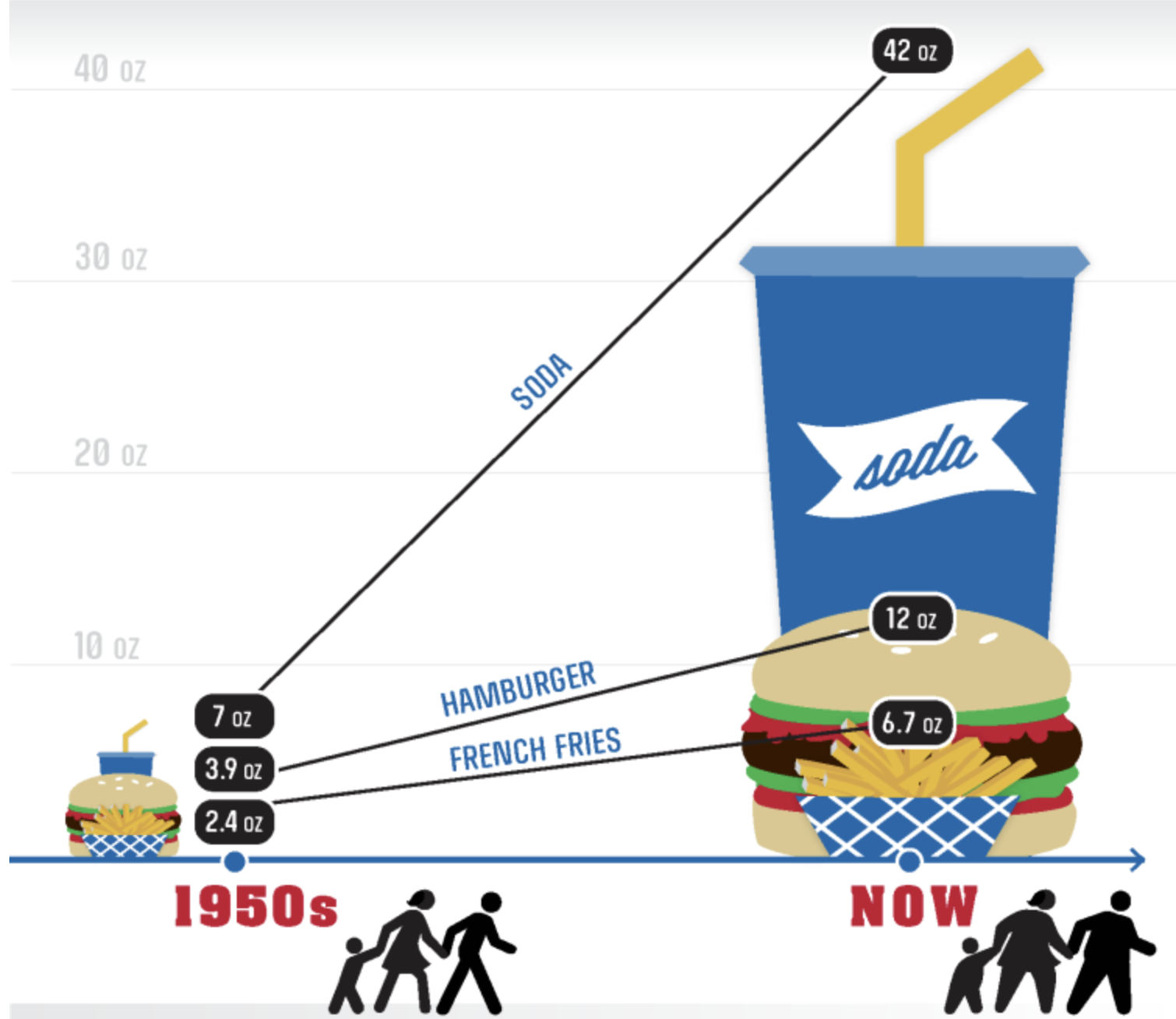
People who eat out consume 200 more calories per day than when they eat at home. Restaurant meals now make up 20% of total daily calories consumed in the US. These meals are often loaded with sodium, fat and added sugar. One study showed that fewer than 0.1% of restaurant meals consumed were of “ideal quality” according to American Heart Association.
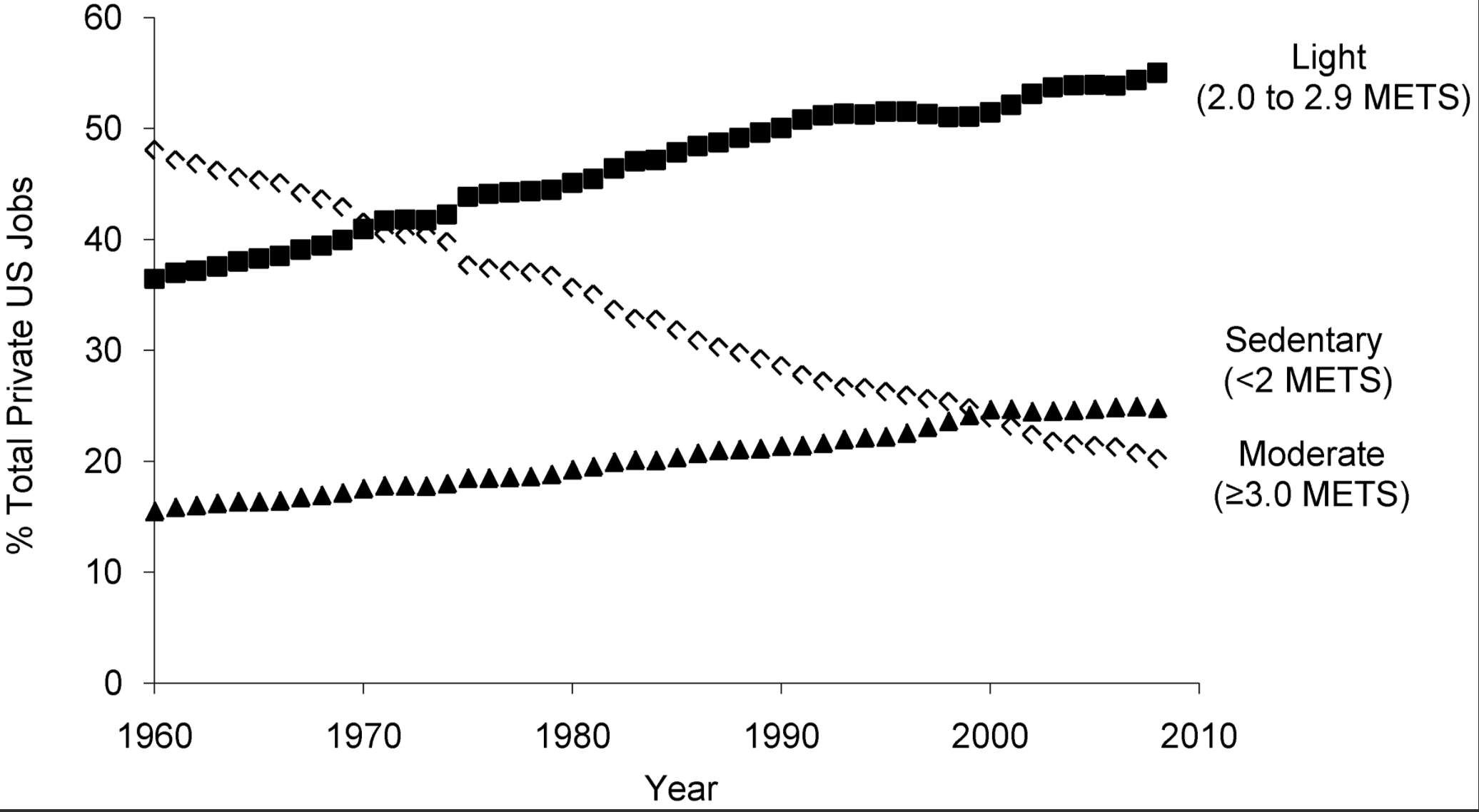
Since 1960 moderate activity jobs have decreased while sedentary and light activity jobs have increased. This accounts for over 100 fewer calories burned per day.
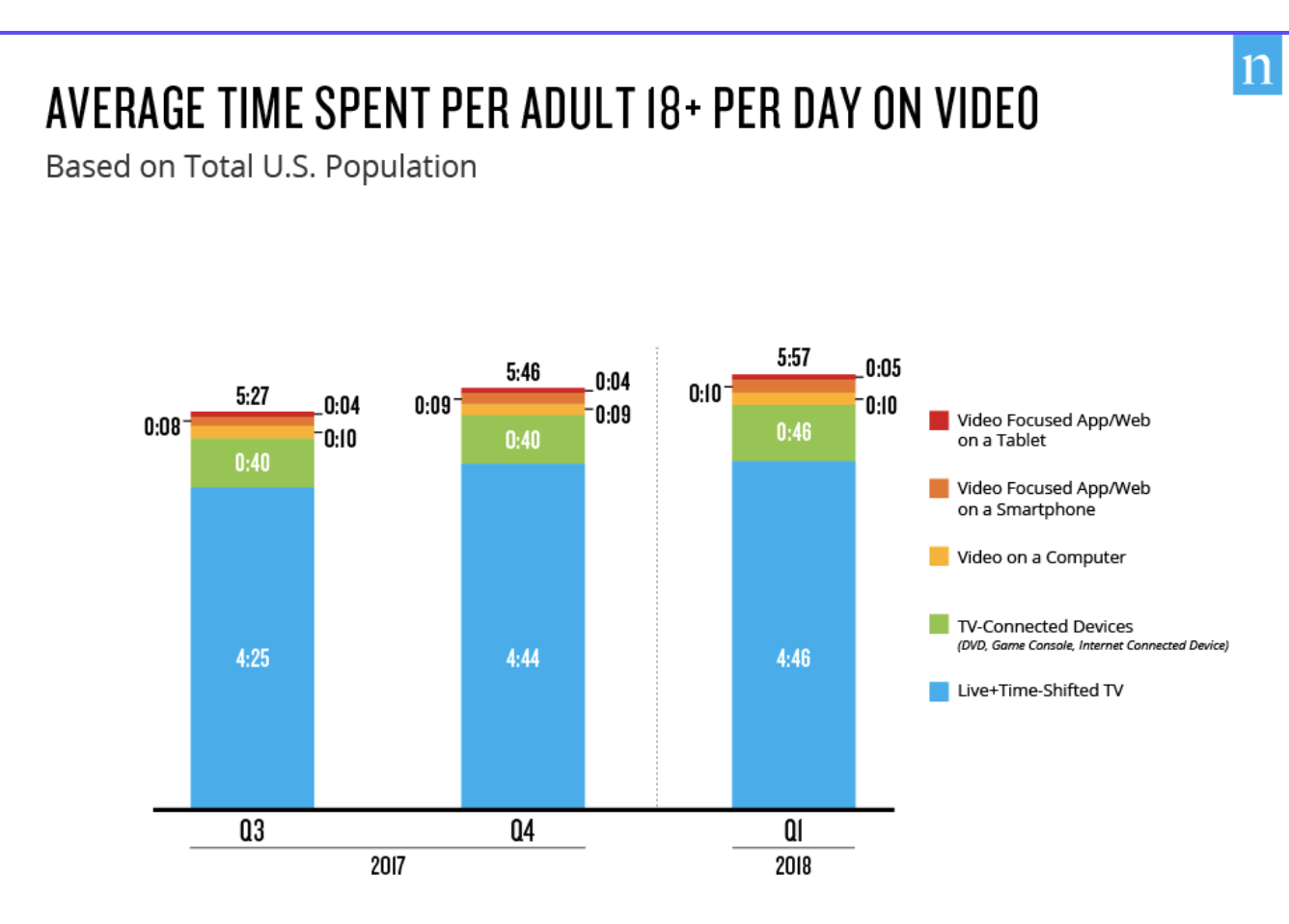
U.S. adults spend almost 6 hours a day watching video. Average time spent on all media (including social media, web, and gaming) is now over 11 hours per day.
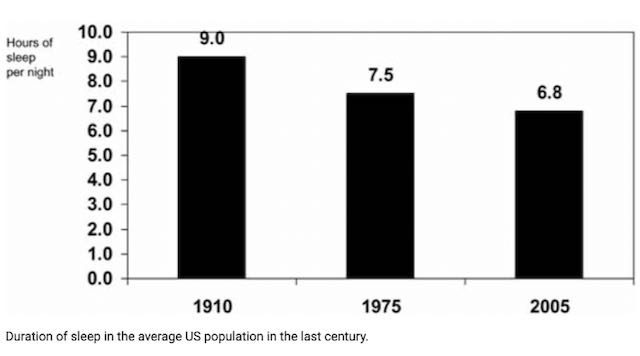
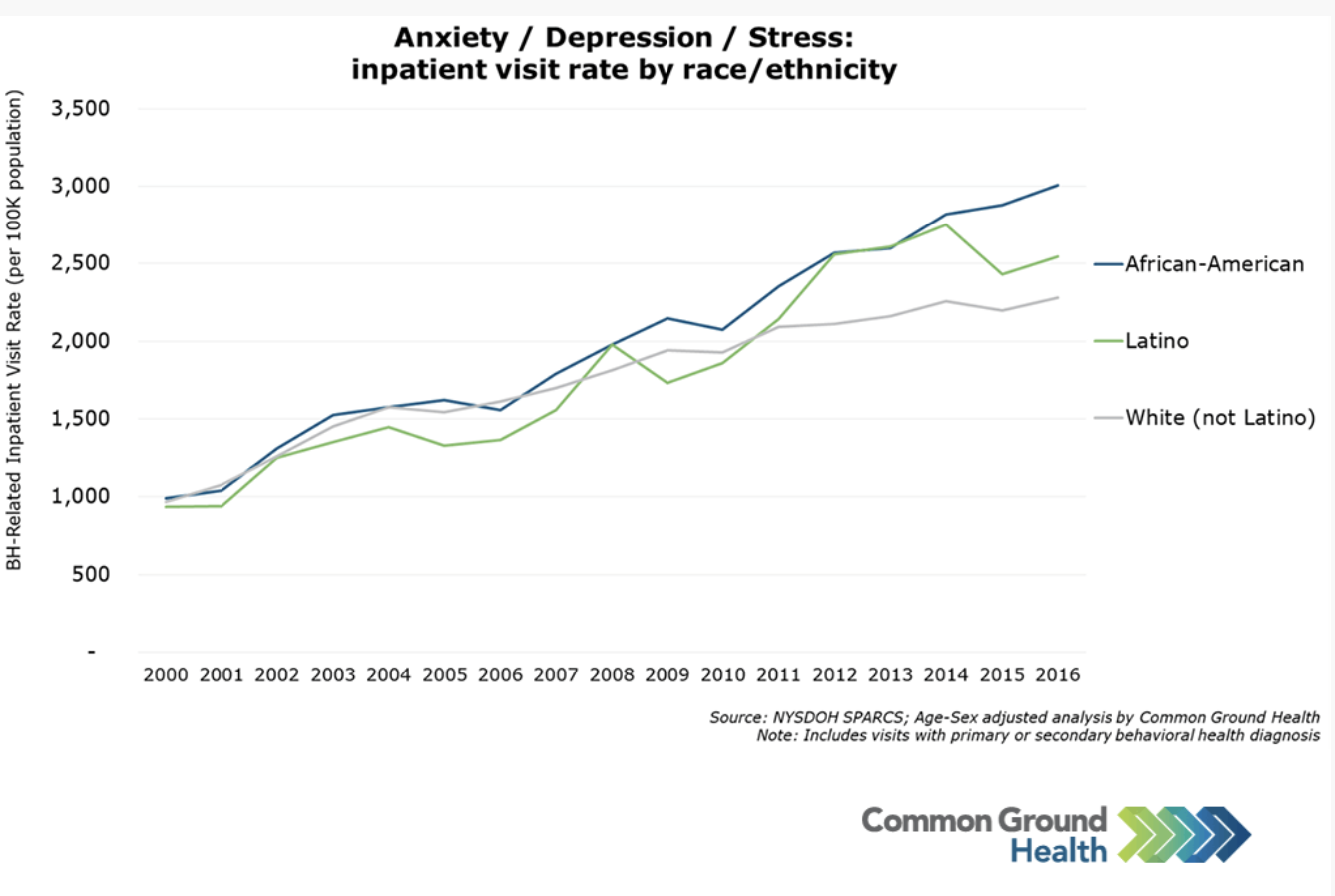
We are also less rested and more stressed than in the past. These issues alter our hormonal environment in ways that make it more difficult to eat healthily and exercise.
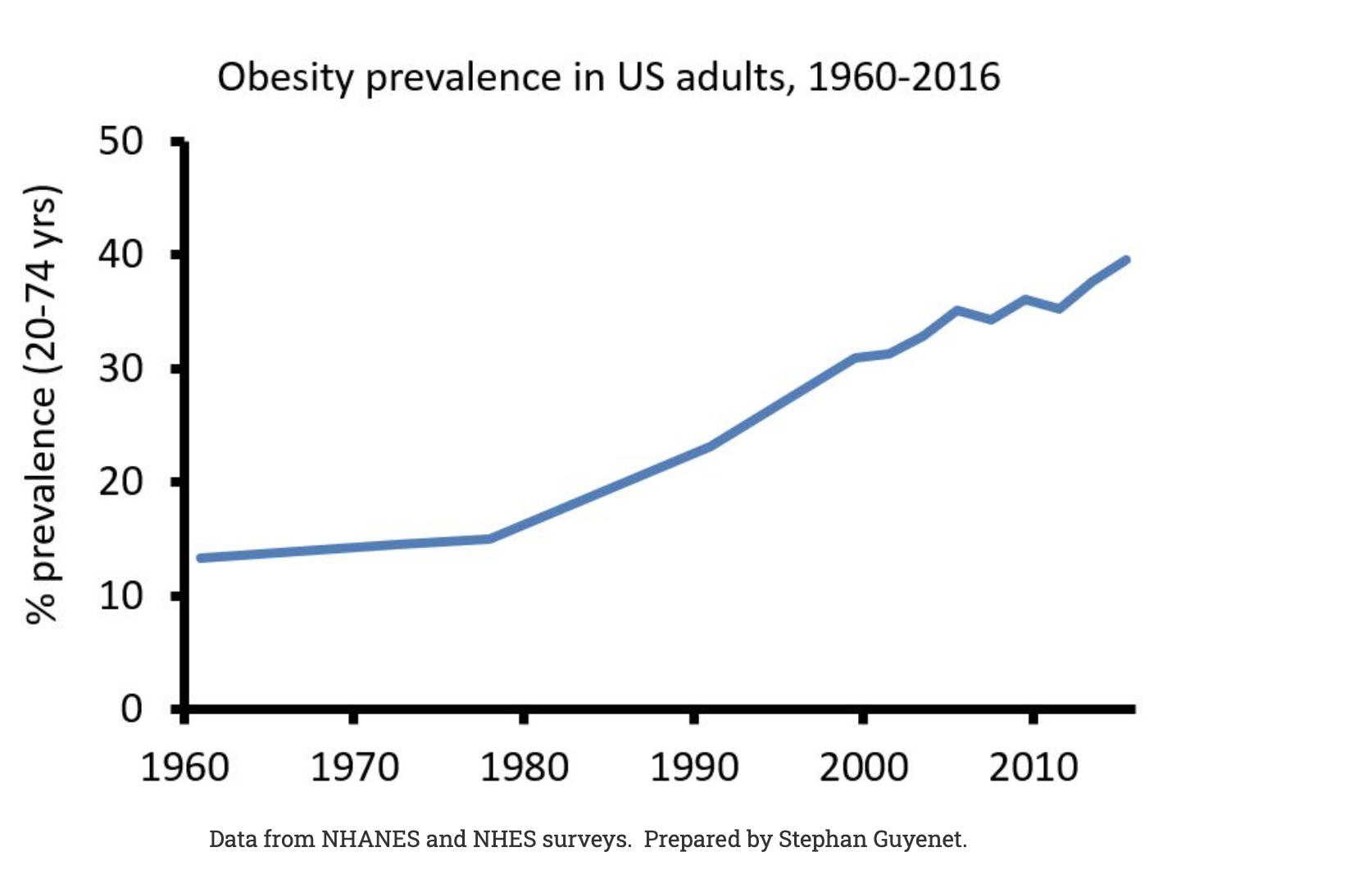
The modern world is an environment that encourages inactivity and overconsumption. It’s an environment where obesity and chronic disease have become the new normal.
Behavioral interventions offer a proven solution.
The US Preventative Service Task Force recommends that clinicians refer adults with a body mass index (BMI) of 30 or higher to intensive, multicomponent behavioral interventions.
Behavioral interventions empower people with skills to overcome environmental obstacles.
These programs help people to set personalized goals to gradually improve diet, and physical activity and build sustainable healthy habits for life.
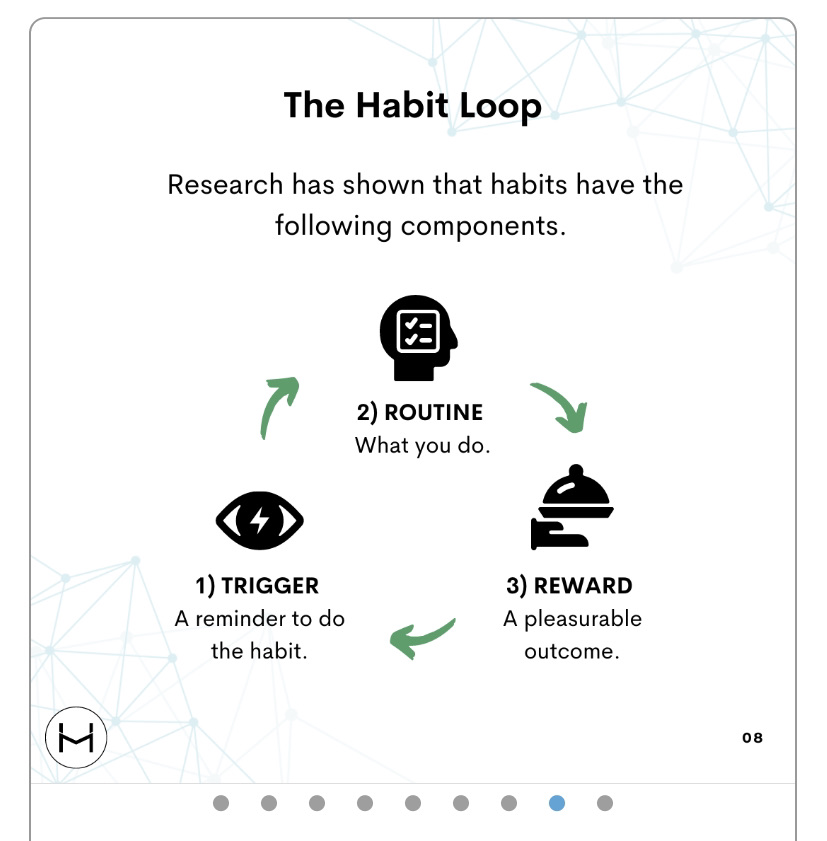
What are the core components of behavioral interventions?
Decades of research have shown that successful programs have 4 common features.
Having participants set a health goal (like a weight loss amount) is a critical foundational element in successful programs. This has been cited as a success driver in meta-analysis of both weight loss and diabetes prevention programs. While participants may choose to change their goal at some point, setting a goal initially indicates a starting point for their journey and helps them consider whether their actions are consistent with the goal they’ve selected.
Clients can set health goals for weight, body fat and circumferences. They are then able to set behavior targets (with input from their coach) to help them achieve these goals.
A curriculum on how to eat, exercise and sustain healthy habits in a challenging environment is another foundational element in successful programs. One of the most widely studied behavior change curriculas is The Diabetes Prevention Program funded by NIH in 1996. Participants in this program showed a 58% reduction in the rate of diabetes in the first 3 years after completion. Follow up studies demonstrated long term behavior change with lower diabetes risk in participants 15 years after program completion. This program is now delivered nationally at over 1500 sites, and the curriculum has been adapted as the basis of many other behavior change programs.
The coaching interface comes with evidence based lessons on nutrition, exercise, health, and behavior change. These cover core topics featured in the National Diabetes Prevention Program curricula, but are condensed to be engaging like social media.
To maximize flexibility, coaches can easily create their own lessons by uploading images or can link to videos, podcasts and other resources on the web.
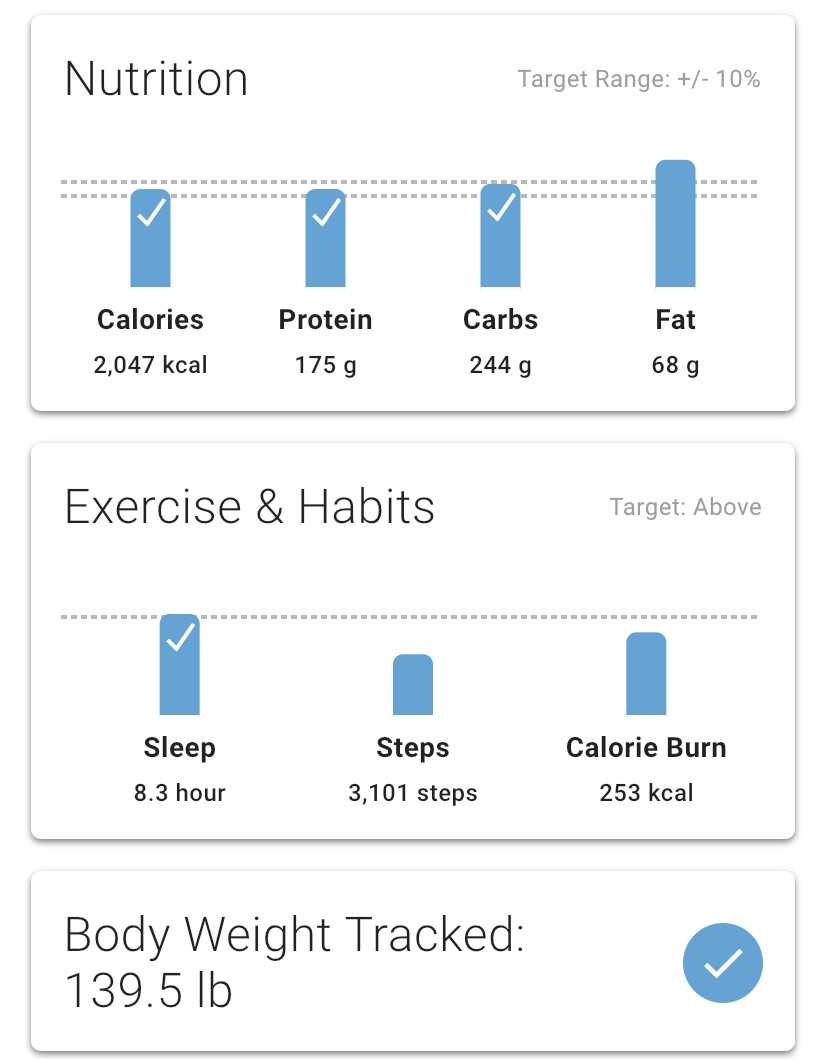
Participants can self-monitor nutrition, steps, calorie burn, sleep, weight, and body fat through any app, or connected device that integrates with Apple Health or Google Fit.
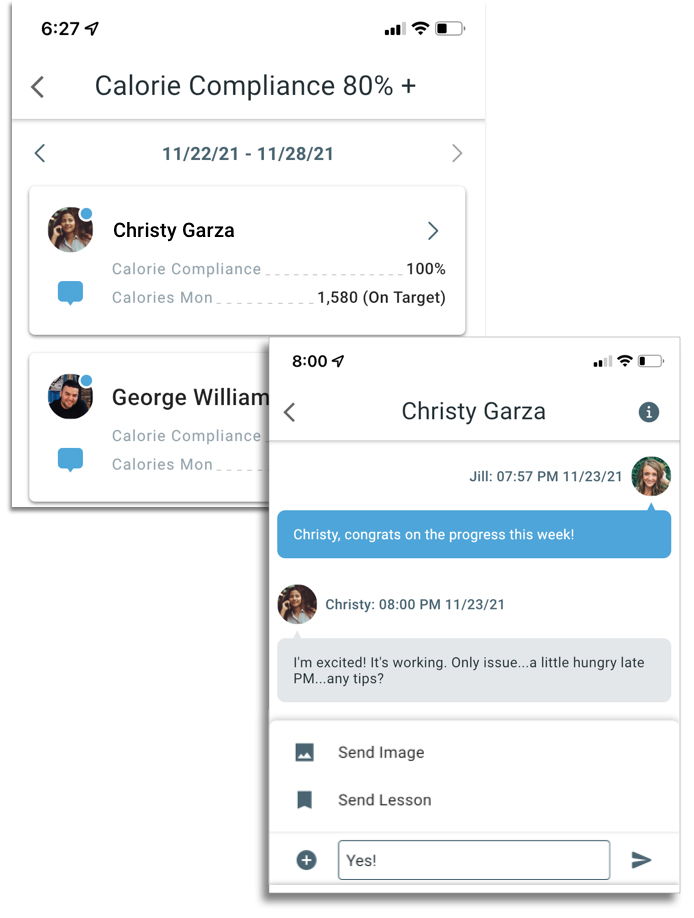
Health Mentor was built to enable this type of coaching. Coaches can efficiently monitor diet, sleep, and exercise for every client from a single dashboard. With a single tap they can filter to see lists of clients who are meeting or struggling with behavior goals. With an additional tap they can message clients to encourage self-monitoring, and provide accountability. When needed, they can follow up with evidence-based lessons from the integrated content library as easily as sending an emoji.